|
|
Craniosynostosis
Premature fusion of one or more of the cranial sutures
General Considerations
- Premature fusion of one or more of the cranial sutures
- Can be primary, resulting from a defect in ossification, or
- Secondary (more often) from failure of growth of the brain
- Brain growth is the major factor in keeping sutures open
- The head shape is frequently abnormal
- The sagittal suture is affected most commonly (50-60%), followed by the coronal, metopic and lambdoid
- Skull growth is restricted perpendicular to the orientation of the suture
Name of Skull Deformity from Craniosynostosis |
Suture(s) Fused Early |
Type of Skull Deformity |
Sagittal suture |
Scaphocephaly (most common) |
One coronal suture |
Anterior plagiocephaly |
Both coronal sutures |
Brachycephaly |
One lambdoid suture |
Posterior plagiocephaly |
Metopic suture |
Trigonocephaly |
All skull sutures and basilar skull sutures |
Oxycephaly |
Fusion of all sutures except metopic and squamosal |
Kleeblattschadel (Cloverleaf skull) |
- Scaphocephaly is most common form
- Occurs more often in premature infants
- Head is elongated from front to back
- Brachycephaly produces a wider skull that is shorter from front to back
- Often part of other syndromes
- May be associated with developmental abnormalities of the face
- Posterior plagiocephaly is more often due to positional molding from sleeping on back than craniosynostosis
- Trigonocephaly produces a triangular-shaped forehead
Clinical Findings
- Becomes evident when child grows (0-18 months)
- Cosmetic deformity
- Elevated intracranial pressure (usually with multiple sutures fusing)
- Neurodevelopmental delay from lack of brain growth in secondary form
Imaging Findings
- Simple (one suture) or compound (complex) when more than one suture
- Skull radiographs are usually diagnostic
- Fused suture lines will be closed and/or sclerotic and ridged
Differential Diagnosis
Treatment
- Surgery may be performed for cosmetic reasons when 1-2 sutures are involved
- Surgery may also be performed to relieve elevated intracranial pressure
Complications
- Increased intracranial pressure if multiple sutures fuse may occur with primary craniosynostosis
- Failure of growth of brain results in microcephaly in secondary craniosynostosis
- May be associated with other syndromes such as Crouzon, Apert, Chotzen, Pfeiffer or Carpenter syndromes
- Secondary craniosynostosis may be associated with hyperthyroidism, hypophosphatemia, vitamin D deficiency, renal osteodystrophy, hypercalcemia, rickets, sickle cell disease or thalassemia
Prognosis
- Primary, single-suture craniosynostosis patients tend to do very well
- In secondary form, prognosis is dependent on underlying cause

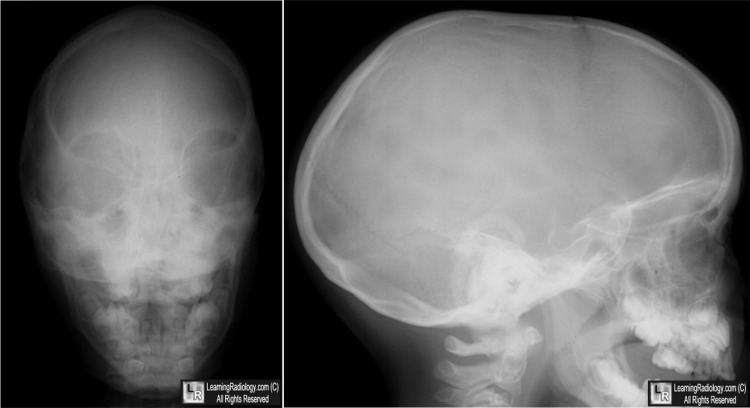
Scaphocephaly. There is premature fusion of the sagittal suture as shown by the line of sclerosis and
ridging at the site of what should be an open suture (white arrow) resulting in a restriction of growth
perpendicular to the suture and an exaggeration of growth parallel to it (scaphocephaly).
The coronal (black arrow) and lambdoid sutures (yellow arrow) are still open.
For this same photo without the arrows, click here
For more information, click on the link if you see this icon 
Pediatric craniosynostosis. eMedicine. R D Sheth, BJ Iskandar, IM Heger, S Roy.
|
|
|

{kind=link}